Mosquito-borne Arboviruses of Virginia
ID
ENTO-535NP
Introduction
Arboviruses (arthropod-borne viruses) are an important cause of illness throughout the world. Mosquitoes and ticks are the key arthropod groups involved in transmitting such vector-borne diseases.
In the Commonwealth of Virginia, there are 58 known species of mosquitoes, comprising nine genera, of which many can act as vectors of viral disease (Harrison et al. 2016). Here we summarize several mosquito-borne viruses circulating in Virginia including West Nile virus, La Crosse virus, St. Louis encephalitis virus, Eastern Equine encephalitis virus, and Jamestown Canyon virus. Treatment for many arboviruses is currently limited to supportive therapy to relieve symptoms, and protection against mosquito bites is the best way to avoid infection.
West Nile virus
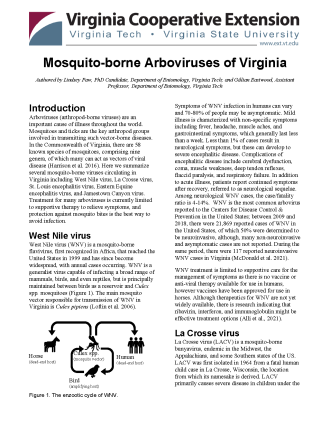
West Nile virus (WNV) is a mosquito-borne flavivirus, first recognized in Africa, that reached the United States in 1999 and has since become widespread, with annual cases occurring. WNV is a generalist virus capable of infecting a broad range of mammals, birds, and even reptiles, but is principally maintained between birds as a reservoir and Culex spp. mosquitoes (Figure 1). The main mosquito vector responsible for transmission of WNV in Virginia is Culex pipiens (Loftin et al. 2006).
Symptoms of WNV infection in humans can vary and 70-80% of people may be asymptomatic. Mild illness is characterized with non-specific symptoms including fever, headache, muscle aches, and gastrointestinal symptoms, which generally last less than a week. Less than 1% of cases result in neurological symptoms, but these can develop to severe encephalitic disease. Complications of encephalitic disease include cerebral dysfunction, coma, muscle weakness, deep tendon reflexes, flaccid paralysis, and respiratory failure. In addition to acute illness, patients report continued symptoms after recovery, referred to as neurological sequelae. Among neurological WNV cases, the case/fatality ratio is 4-14%. WNV is the most common arbovirus reported to the Centers for Disease Control & Prevention in the United States; between 2009 and 2018, there were 21,869 reported cases of WNV in the United States, of which 50% were determined to be neuroinvasive, although, many non-neuroinvasive and asymptomatic cases are not reported. During the same period, there were 117 reported neuroinvasive WNV cases in Virginia (McDonald et al. 2021).
WNV treatment is limited to supportive care for the management of symptoms as there is no vaccine or anti-viral therapy available for use in humans, however vaccines have been approved for use in horses. Although therapeutics for WNV are not yet widely available, there is research indicating that ribavirin, interferon, and immunoglobulin might be effective treatment options (Alli et al., 2021).
La Crosse virus
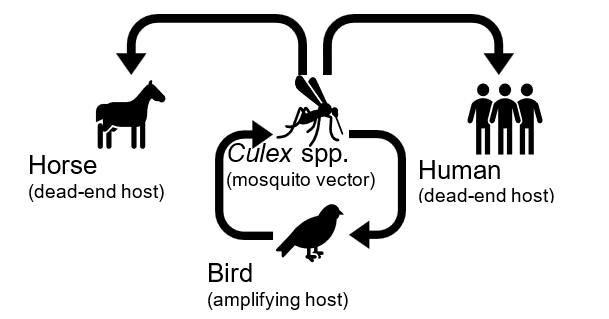
La Crosse virus (LACV) is a mosquito-borne bunyavirus, endemic in the Midwest, the Appalachians, and some Southern states of the US. LACV was first isolated in 1964 from a fatal human child case in La Crosse, Wisconsin, the location from which its namesake is derived. LACV primarily causes severe disease in children under the age of 16 and is the leading cause of pediatric encephalitis in the United States. LACV is maintained in nature via an enzootic cycle between Aedes triseriatus mosquitoes (although other Aedes spp. mosquitoes can act as vectors) and sciurid species (i.e., squirrels and chipmunks) as vertebrate reservoir hosts (CDC, 2020) (Figure 2).
Clinical cases of LACV infection can manifest as asymptomatic (no symptoms), mild (characterized by headaches and fever), or become neuroinvasive. Symptoms of severe neuroinvasive cases include seizures, coma, and paralysis (McJunkin et al. 2001).
In Virginia, between 2011 and 2020, nine LACV cases were reported to CDC. LACV is now considered an emerging threat in the Appalachian region; surrounding states, North Carolina, Tennessee, and West Virginia have reported high numbers of LACV cases so a travel risk may exist. Treatment for LACV is currently limited to supportive therapy to relieve symptoms, but there are currently no treatments that target the virus itself (CDC, 2022).
St. Louis Encephalitis virus
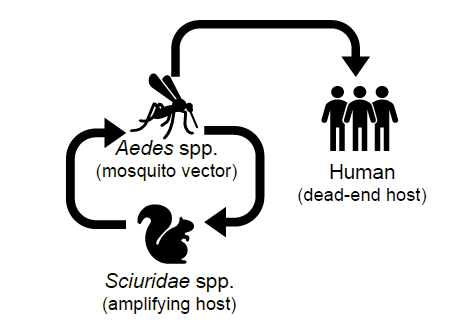
St. Louis encephalitis virus (SLEV) is a mosquito-borne flavivirus vectored by the Culex genus of mosquitoes, and utilizes birds as reservoir hosts (Figure 3). SLEV is widespread throughout the Americas, but most outbreaks in the USA have occurred sporadically in the Southwest (CDC, 2021; Diaz et al. 2018).
Symptomatic cases of SLEV are characterized by fever, headache, dizziness, weakness, and nausea. In severe cases, SLEV can infect the central nervous system resulting in encephalitis and/or meningitis along with confusion, disorientation, tremors, dizziness, stiff neck, coma, and death (CDC, 2022).
While there is evidence that SLEV is circulating in Virginia (preliminary data from the Eastwood Lab at VT), knowledge of human cases has been limited in the years since WNV emergence; no cases of SLEV were reported to the CDC by Virginia between 2011-2020. There is no specific treatment for SLEV, but supportive care can help alleviate symptoms (CDC, 2022).
Eastern Equine Encephalitis virus
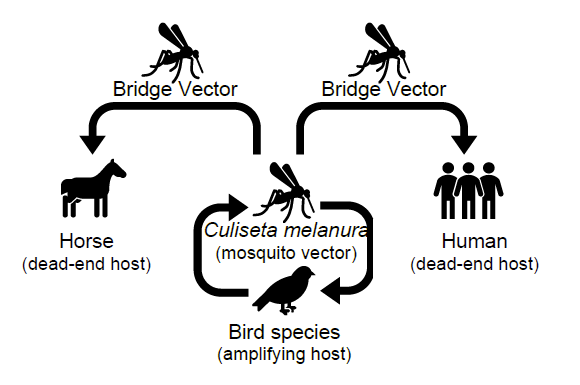
Eastern equine encephalitis virus (EEEV) is a rare but serious mosquito-borne alphavirus, prevalent along the Eastern seaboard of the US with cases primarily occurring in the Northeast and Midwest. EEEV maintains an enzootic cycle utilizing Culiseta melanura mosquitoes as vectors, and birds as reservoir species. Humans and horses are ‘dead-end hosts’, but gain infection from the involvement of a “bridge vector” mosquito, which leads to spillover of the virus outside its usual cycle (CDC, 2021) (Fig 4).
The majority (90%) of EEEV infections are asymptomatic, but symptomatic cases exhibit non-specific signs such as fever, headaches, muscle aches, and nausea, 4-10 days after a mosquito bite. In more severe encephalitic cases, neurologic damage can persist, or death occur in one in three such cases (Morens, Folkers, & Fauci, 2019).
Between 2011 and 2020, one EEEV case was reported in Virginia, which occurred on the eastern side of the state; EEEV transmission is often associated with swamp lands that exist in the eastern part of the state (Culiseta spp. vector habitat). The virus is present also in neighboring states. There is no current treatment for EEEV infection and medical care is limited to supportive care that can help alleviate symptomatic discomfort (CDC, 2021).
Jamestown Canyon virus
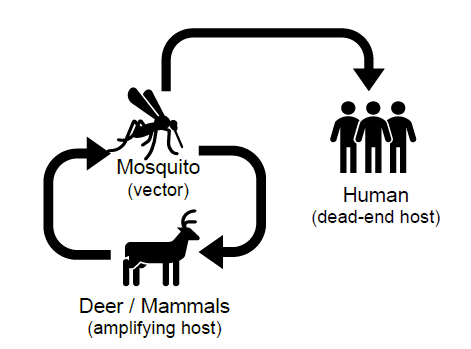
Jamestown Canyon virus (JCV) is a mosquito-borne orthobunyavirus, related to LACV, which is widespread and under-recognized throughout the United States. JCV is maintained in an enzootic cycle via a wide range of different mosquito species and can infect a variety of mammalian reservoir hosts, primarily white-tailed deer (Pastula et al. 2015; Kinsella et al. 2020) (Figure 5).
Clinical cases of JCV often present as a non-specific illness characterized by fever, fatigue, and headache, sometimes respiratory symptoms, although many cases are asymptomatic. In more severe illness, JCV infection can result in encephalitis, confusion, seizures, among other neurologic symptoms (CDC, 2022).
Although no JCV cases were reported in Virginia between 2011 and 2020, the virus has been detected in mosquitoes, therefore a risk of infection exists in the Commonwealth. As with the other viruses explored here, there is no specific treatment to treat JCV clinical cases other than supportive care to relieve resulting symptoms (CDC, 2021; CDC, 2022).
Surveillance, Control, and Prevention of mosquito-borne arboviruses
Surveillance: Local communities and governments conduct various levels of mosquito surveillance and control. In Virginia, vector control is primarily conducted at the county level. Surveillance for arboviruses can provide initial indication that viruses are circulating locally and may present a risk to human health. Testing vertebrate hosts (including sentinels) and mosquito vectors for evidence of viral infection can be an effective management practice to reduce cases of mosquito-borne arboviruses by timely determination of risks and implementing appropriate countermeasures.
Control: Mosquito control is the primary method for limiting the disease burden from arboviral infections. Mosquito control can take many forms, including primarily reducing the availability of breeding habitats to limit reproduction by mosquitoes. This is something that you can ensure around your property, for example: old tires, birdbaths, and other water-holding containers should be dumped to prevent mosquitoes from breeding in the water. Larvicides may be used to target immature mosquitoes, and finally, adulticides, such as spraying applications, may be deployed.
Prevention: The best method to protect yourself and your family is to use personal protection including wearing clothing that covers the arms and legs and using insect repellents when outdoors. Around the home, it is recommended that windows be screened to prevent the entry of mosquitoes into the home, and any water-holding containers around the home are regularly emptied or discarded (CDC, 2022).
References
Alli, A., J.F. Ortiz, Atoot, A., Atoot, A., and P.W. Millhouse. 2021. “Management of West Nile Encephalitis: An Uncommon Complication of West Nile Virus.” Cureus 2.
Diaz, A., L.L. Coffey, N. Burkett-Cadena, & J.F. Day. 2018. Reemergence of St. Louis Encephalitis Virus in the Americas. Emerging Infectious Diseases, 24(12), 2150-2157.
“Epidemiology & Geographic Distribution | La Crosse Encephalitis | CDC.” 2020. November 20, 2020. https://www.cdc.gov/lac/tech/epi.html.
Harrison, B.A, B.D. Byrd, C.B. Sither, and P.B. Whitt. 2016. The Mosquitoes of the Mid-Atlantic Region: An Identification Guide. Mosquito and Vector-borne Infectious Diseases Laboratory Publication 2016-1, Western Carolina University, Cullowhee, NC.
Kinsella, C.M., M.L. Paras, S. Smole, S. Mehta, V. Ganesh, L.H. Chen, D.P. McQuillen, et al. 2020. “Jamestown Canyon Virus in Massachusetts: Clinical Case Series and Vector Screening.” Emerging Microbes & Infections 9 (1): 903–12.
Loftin, K.C., A.A. Diallo, M.W. Herbert, P.G. Phaltankar, C. Yuan, N. Grefe, A. Flemming et al. 2006. “Five-Year Surveillance of West Nile and Eastern Equine Encephalitis Viruses in Southeastern Virginia.” Journal of Environmental Health 68 (9): 33–40.
McDonald, E., S. Mathis, S.W. Martin, J.E. Staples, M. Fischer, and N.P. Lindsey. 2021. “Surveillance for West Nile Virus Disease — United States, 2009–2018.” American Journal of Transplantation 21 (5): 1959–74.
McJunkin, J.E., E.C. de los Reyes, J.E. Irazuzta, M.J. Caceres, R.R. Khan, L.L. Minnich, K.D. Fu, G.D. Lovett, T. Tsai, and A. Thompson. 2001. “La Crosse Encephalitis in Children.” New Enlgand Journal of Medicine 344: 801–7.
Morens, D.M., G.K. Folkers, and A.S. Fauci. 2019. “Eastern Equine Encephalitis Virus — Another Emergent Arbovirus in the United States.” New England Journal of Medicine 381 (21): 1989–92.
Pastula, D.M., D.K. Hoang Johnson, J.L. White, A.P. Dupuis, M. Fischer, and J.E. Staples. 2015. “Jamestown Canyon Virus Disease in the United States—2000–2013.” The American Journal of Tropical Medicine and Hygiene 93 (2): 384–89.
“Prevent Mosquito Bites | Mosquitoes | CDC.” 2022. November 2, 2022.
“Statistics & Maps | Eastern Equine Encephalitis | CDC.” 2021. December 16, 2021.
“Statistics & Maps | Jamestown Canyon Virus | CDC.” 2021. December 14, 2021.
“Statistics & Maps | La Crosse Encephalitis | CDC.” 2022. January 7, 2022.
“Statistics & Maps | St. Louis Encephalitis | CDC.” 2021. December 17, 2021.
“Symptoms, Diagnosis, & Treatment | Jamestown Canyon Virus | CDC.” 2022. October 13, 2022.
“Symptoms, Diagnosis, & Treatment | La Crosse Encephalitis | CDC.” 2022. January 7, 2022.
“Symptoms, Diagnosis, & Treatment | St. Louis Encephalitis | CDC.” 2022. October 14, 2022.
Virginia Cooperative Extension materials are available for public use, reprint, or citation without further permission, provided the use includes credit to the author and to Virginia Cooperative Extension, Virginia Tech, and Virginia State University.
Virginia Cooperative Extension is a partnership of Virginia Tech, Virginia State University, the U.S. Department of Agriculture (USDA), and local governments, and is an equal opportunity employer. For the full non-discrimination statement, please visit ext.vt.edu/accessibility.
Publication Date
March 10, 2023